Recent polling shows Elizabeth Warren climbing in popularity.1 It’s even been asserted that she will overtake Joe Biden as the Democratic front-runner.2 If Elizabeth Warren won the democratic primary and beat Trump in the general election, what might that presidency look like politically? What would it mean for the economy? What industries might be affected? Below is a look at one of Senator Warren’s many plans, Medicare for All.
Healthcare– Medicare for All
Senator Warren signed on to Senator Sanders’ Medicare For All Act (M4A) back in 2017.3 But it wasn’t until June of 2019 that she was explicit in her support for the M4A 2109 Act put forward by Senator Sanders.4 Her own proposal is based on Senator Sanders M4A 2019 Act and like any policy, the devil is in the details. The plans are essentially the same in scope and benefits offered. The difference is how they plan to pay for it. Senator Sanders has broadly outlined some tax increases, including taxes on the middle class, to pay for his proposal. While Senator Warren has taken the unusual step of providing specific details of exactly how the program will work, the costs involved, and how to pay for it. This article summarizes those details and discusses the impact on the economy, consumers, industries, as well as the political viability of the proposal.
First, a short review of some healthcare terminology and a baseline of the current state of the US healthcare system. According to the Urban Institute, the difference between the National Health Spending (NHS) and Federal Health Spending (FHS) is an important distinction and should not be confused when making policy comparisons.5 The NHS is all of the money spent on healthcare including that by the US government, while Federal Health Spending (FHS) is the amount spent by just the US government on “Medicare, Medicaid, the Children’s Health Insurance Program, Affordable Care Act, marketplace premium subsidies, the Veterans Administration, US Department of Defense health care programs, support for health care professionals and hospitals providing uncompensated care, as well as other federal programs.”5 Furthermore, it is possible for the FHS to increase while the NHS decreases. For example, the NHS could go down if the US government takes over health services currently paid for by others outside of the government while also reducing the cost of providing those services. However, Urban cautions, there are limits. For example, an increase in the use of services can outweigh any cost reduction for services provided.5
In 2017, the NHS totaled $3.5T.6 Over the next 10 years (2019-2029), the NHS will total over $52.5T (CMS Projections using the average growth for past 8 years of 5.7% in years 2028 and 2029) and of that, US residents would pay about $11T.7 On a per capita basis, US consumers pay over $10,000 in health expenditures, more than double what Canadians pay ($4,826) and almost double the average of all comparable countries ($5,280).8 Even more pronounced is the difference in private healthcare expenditures when compared to other countries. The US private sector pays almost triple that of comparable countries.8 Yet, on average 29M people per month went uninsured in 2018.9 Furthermore, US women are greater than 4 times more likely to die from complications during childbirth compared to women in other countries. Finally, the US ranks last (2016) when it comes to deaths from diseases that could have been prevented with regular care (Amenable Mortality).8 Those facts are not in dispute. The US pays the most for healthcare but doesn’t provide the best care nor does it cover all of its citizens. In fact, the US ranks last in the world.10
Assessing the Plan
Under Senator Warren’s M4A plan, all individuals in the United States would be covered, including undocumented migrants. “Medicare for All is the best way to give every single person in this country a guarantee of high-quality health care. Everybody is covered.”11 Additionally, the benefits not only include basic health, but also long-term care, at-home care, community care, mental health, dental, vision, and hearing. There would be no deductibles, no premiums, and no co-pays (no cost-sharing).7
In an unusual political move, Senator Warren released an enormous amount of detail about her M4A policy including how she plans to pay for it as well as several expert research studies about the costs and benefits of the policy.12 Two of those experts were Dr. Donald Berwick, Former Administrator of the Centers for Medicare and Medicaid Services (CMS), and Simon Johnson, Chief Economist at the International Monetary Fund (IMF). They used data from an Urban Institute study13 as a benchmark to apply Senator Warren’s cost-saving initiatives.14 The Urban Institute study used data from 4 microsimulation models maintained and updated by Urban. It is not easy to say if these are the best microsimulation models. However, it is an appropriate way to model something as large and complex as the move to single-payer healthcare. Additionally, the Urban study produced some of the highest cost estimates for implementing a single-payer program.14 It was therefore considered a conservative estimate of costs. However, it is important to note that the Urban Institute’s models assume that the proposals are fully implemented and running at a “steady state” at the time of the simulation.13 Obviously this does not account for costs associated with planning and implementing the program, nor reassigning of displaced workers. Although, Senator Warren has promised a transition plan in the near future.7
By Senator Warren and others’ accounts,15 the NHS would total less than the $52.5T already projected by CMS for the next ten years. As would be expected, however, Federal Health Spending (FHS) would go up. The US government is absorbing the costs normally spread over individuals, businesses, and state and local governments as well as adding benefits and millions of more subscribers. The Urban Institute estimated an additional $34T in FHS above the currently projected $17T for a single-payer health plan similar to Senator Warren’s M4A plan.5 According to the Urban Institute, it is possible for the NHS to drop while the FHS rises. However, as noted earlier, there are limits. The US is adding more services and more subscribers, the very thing Urban cautioned would be difficult to counter in the NHS. In fact, Urban determined that the increased benefits, health services usage, and the addition of millions of more participants outweighed the benefits of reduced pricing (paying providers at medicare prices), reduced prescription drug fees, and reduced administrative costs.5 Senator Warren’s plan then went further with more government reforms that lower costs in areas Urban didn’t model.
In October of 2019, Berwick et al. applied Senator Warren’s cost savings policies to the Urban Institutes numbers.14 According to the Urban Institute, FHS rises an additional $34T to $51T over the next ten years. After the cost savings are applied that $34T is reduced to $20.5T (see Table 1). However, the total FHS over that time period would be $37.5T, which is the original $17T plus the $20.5 trillion.
Paying For It
Senator Warren has over 50 comprehensive and connected plans for overhauling the US Government, economy, markets, industries, immigration, to name a few. Many of which M4A depends upon before being legislated and any one of which would be a challenge to pass even in a Democratic majority house and senate. This rather fragile thread for funding M4A has two fronts, revenue generation, and cost savings. The revenue sources for making up that $20.5T are 7 fold:
- Employer contributions: Instead of paying premiums to insurers, companies would send an estimated $8.8 trillion over 10 years to the federal government as an “Employer Medicare Contribution.” According to Senator Warren, in the first year of M4A, businesses would pay 2% less than whatever their average per employee premiums was for the years before M4A implementation. For companies not providing insurance to employees, they will pay $500 per uninsured employee. Small businesses and self-employed (under a certain income threshold) are exempt; Unionized firms (and any other firm that can pass savings along to employees) can save more if they pass the savings on to their employees.
- Taxes on the wealthy:
- Ultra Millionaire Tax – 2% on wealth above $50M
- Billionaire Tax – 6% on net worth above $1 billion.
- The wealthiest 1% would be taxed on capital gains as income, annually regardless of any sale.
- Reducing tax evasion: Warren argues that she can collect $2.3 trillion by empowering the Internal Revenue Service to crack down on tax evasion and fraud, redirecting the agency’s focus to high-income earners.
- Financial sector taxes: Senator Warren would impose a financial transaction tax of 0.1% on the sale of stocks, bonds, and derivatives.
- Foreign corporations tax: Foreign corporations would pay the difference between 35% of revenue and their home tax rate (where they book their profits) without deferment allowed.
- Taxing additional take-home pay: Since employees would no longer have to pay their share of health care premiums, their take-home pay would go up, thus additional tax revenue.
- Comprehensive immigration reform: This will boost the tax-paying population and result in additional tax revenue but this means providing more care costs less than the revenue generated by taxes. Senator Warren claims this would generate another $400 billion.
- Pentagon’s Overseas Contingency Operations Fund: what was supposed to be a temporary way to pay for the Iraq war became a catch-all slush fund for pet projects that bypasses the normal appropriations process. Eliminating this fund would direct another $798B to Medicare for All over a ten year period.16
(source: https://elizabethwarren.com/plans/paying-for-m4a)
In addition to the revenue sources, Senator Warren has outlined several cost-saving measures.
By the plan’s very nature– cut costs, increase efficiency– people will lose jobs, about 2 million jobs.17 According to Dr. Robert Pollin of the University of Massachusetts’ Political Economic Research Institute, “most of the 2-million job losses would hit administrative positions – half among insurers half among doctors’ offices.”18 Other losers in this reform would be “drug and device sales reps.” KHN also noted that while some jobs would be lost, “reform would ultimately redirect resources in ways that are good for the economy” as well, as in creating new jobs. For example, some healthcare positions would be in higher demand, physicians, nurse practitioners, physicians’ assistants, and personal care attendants.18
The insurers lose more than just their administrators though. Private health insurers for the most part would go out of business in the US. There is a chance while trying to legislate the proposal that insurers are allowed to continue on in some capacity. For example, health insurance for those who want to pay for it, similar to Canada or as supplementary insurance. However, this would still be a limited capacity. In either case, we would need a transition plan in place to help those who will lose their jobs and to avoid chaos. As Dr. Pollin explained, “we’re asking health insurers to lose their jobs but before they do, take better care of more people until we switch over.”19 It is a lot to ask.
Cost of Prescription Drugs
A second cost-saving measure in the form of lowering the cost of prescription drugs through several legislative acts; Lower Prescription Drug Costs Now Act, Affordable Drug Manufacturing Act, and the Medicare Negotiation and Competitive Licensing Act. The first two bills allow the government to negotiate directly with pharmaceutical companies. If negotiations fail, HHS can license the drug to a new manufacturer, regardless of patent protections, who would pay “reasonable compensation” to the original manufacturer as determined by HHS.20 The second bill allows HHS to disperse public funds to subsidize supply.7 Through this legislation, a new department would be formed within HHS that can “step in” to make generic drugs when no one else wants to, when shortages exist, during price spikes, or when “essential” drugs have high prices.7 It’s also possible for HHS to import from select countries. “Stepping in” requires the government to either establish or contract with manufacturers and suppliers. A solution that would require many resources to establish new plants and supply chains if none exists or finding manufacturers who are set up for each specific drug. It’s also important to note this piece of legislation would need to pass the House and Senate before M4A is passed. Currently, the Trump administration may be paving the way for this as HHS is suing Gilead Sciences over HIV drug patent infringement.21 Lastly, Senator Warren’s modified version of the Lower Prescription Drug Costs Now Act allows HHS to impose a 65% excise tax on gross sales of the costliest brand name or generic drugs. If the manufacturer does not comply, that figure goes up 10% every quarter until it reaches 95%. Drug prices would be capped at 110% of the average price in Australia, Canada, France, Germany, Japan, and the U.K. for the same drug.7 22
Payment Reform
Another cost-saving measure reduces the price that providers can charge the government for services. Hospitals and physicians will be getting paid uniformly less. Hospitals will be paid at 110% of Medicare rates, Rural hospitals higher than that and physicians will be paid at Medicare rates. For physicians, their income for the most part will go down. depending on specialty, anywhere from 9% to 30% (see table 2). However, an expected increase in patient population and a decrease in administrative time means more billable hours for providers so an estimated 9% increase in billable hours to offset some of the decrease in revenue.17 Although, not all physicians are affected equally. Specialists will lose the most, up to 30% of pay for neurosurgeons, while most primary care doctors lose about 9% of income– so a wash for primary care physicians. However, if doctors aren’t doing their own administrative work, then their costs may be reduced further and an additional job would be lost.
Slowing Medical Costs Growth
Senator Warren sees two major factors for reducing healthcare cost growth, lowering prescription drug prices (as noted) and moving to a value-based payment system.7 The value-based payment system is not a new concept and CMS already has several programs in place (see Table 3). The system forces providers to work more efficiently and with an outcome in mind rather than providing more services (current fee-for-service model). The “value” is “derived from measuring health outcomes against the cost of delivering the outcomes.”23
Redirecting Other Public Spending
Under this approach, current state and local governments spending on employee health insurance plans will be redirected into the M4A program resulting in $2.7T in contributions. Additionally, State and local governments will send $3.3T of their current Medicaid and the Children’s Health Insurance Program spending to M4A.7 The total is the $6T reduction from the FHS (Table 2).
While this report is focused on the commercial impacts of the legislation, it is impossible to ignore the impact on individuals. More specifically, impacts on individuals and families with regard to income and spending.
Senator Warren’s plan eliminates out-of-pocket expenses and premiums for individuals thereby putting “$11T back in the pockets of the American people.”12 Americans have a poor track record for saving so much of that $11T will be spent and that’s always good for the economy.
For high-net-worth families, that’s anyone worth more than $50M it’s a slightly different story. It is true that whatever premiums they currently pay will go away, but due to the 2% millionaire tax, anyone worth over $50M will pay an additional $1 million in taxes (that’s using 0.02 x $50M) and anyone worth over $1B will pay 6% in tax—that’s $60M in tax on net worth of $1B. Additionally, with the change to how long-term capital gains are taxed is more complicated. The top 1% of earners, that’s anyone making over $700k annually, will have long-term capital gains taxed as income (37% is the top bracket) and it happens annually regardless of a transaction.24 The messy part is putting together an annual market valuation for your gains, crediting back any losses, then having it change year to year.25
As stated earlier, M4A depends on several large, complex pieces of legislation for funding and cost savings. As such, keeping costs down for such a large complex program is difficult to say the least. Making funding contingent upon the passage of so many other complex and potentially disruptive proposals makes financing near impossible. Furthermore, in the current political environment, these programs are unlikely to move forward or, being optimistic, move forward without changes more tuned to the Republican party line. Consequently, M4A is unlikely to pass. Not only because Republicans would oppose it just on principle but also because many moderate Democrats don’t support it.26 So why propose and embrace such long-shot platforms? It may have more to do with winning over Bernie Sanders’ base than actual beliefs.26
Table 1: Ten-Year Cost Reductions Relative to Urban Institute Projections
|
Source |
Estimated Federal Costs and Cost Savings, 2020-29 (in trillions) |
|
Urban Estimate of Additional Federal Spending |
34.0 |
|
Insurer Administrative Spending |
-1.8 |
|
Prescription Drug Reform |
-1.7 |
|
Comprehensive Payment Reform |
-2.9 |
|
Slowing Medical Costs Growth over Time |
-1.1 |
|
Redirecting Other Public Spending on Health Coverage |
-6.1 |
|
Estimate of New Federal Spending Required |
20.5 |
(Source: https://assets.ctfassets.net/4ubxbgy9463z/2Tg9oB55ICu2vtYBaKKcVr/d124e0eeb128ad3a8d8ab8a6ccae44c0/20191031_Medicare_for_All_Cost_Letter___Appendices_FINAL.pdf)
Table 2 (From PERI Study Appendix A2.2 p132)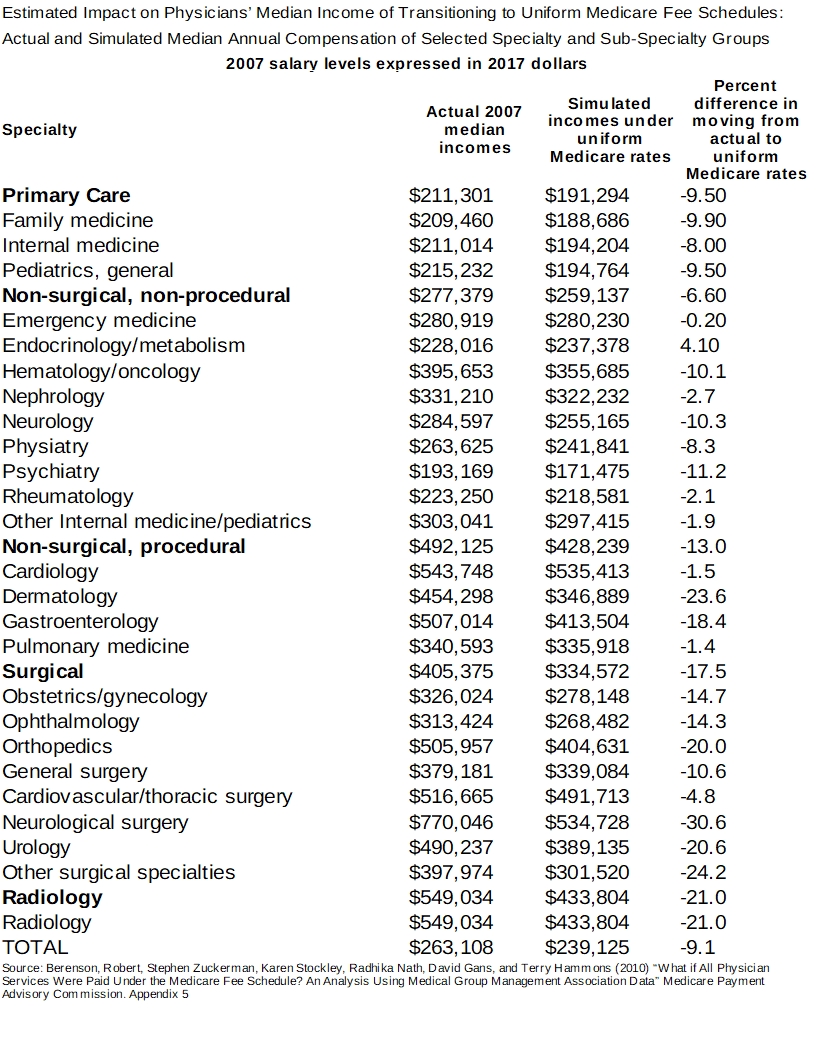
Table 3
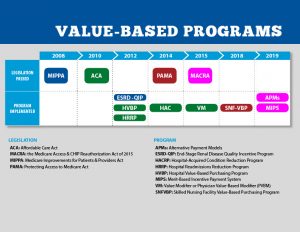
(Source: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/Value-Based-Programs.html)
1. National poll: Biden, Warren, and Sanders locked together at top of primary. POLITICO. https://www.politico.com/news/2019/11/06/national-poll-warren-sanders-biden-lead-066646. Accessed November 14, 2019.
2. Joe Biden won’t win | Spectator USA. https://spectator.us/joe-biden-wont-win/. Accessed October 29, 2019.
3. Marans D, Cohn J. Bernie Sanders Announces Single-Payer Bill With Major Support In Senate. HuffPost. https://www.huffpost.com/entry/bernie-sanders-single-payer-bill-major-support-senate_n_59b87dc1e4b02da0e13d465f. Published 00:00 400AD. Accessed November 5, 2019.
4. Weissmann J. Only Two Democrats Onstage Said They Support Single Payer. That’s Telling. Slate Magazine. https://slate.com/business/2019/06/elizabeth-warren-debate-single-payer-medicare-for-all.html. Published June 27, 2019. Accessed November 14, 2019.
5. Blumberg LJ, Holahan J, Simpson M. Don’t Confuse Changes in Federal Health Spending with National Health Spending. Urban Institute. https://www.urban.org/urban-wire/dont-confuse-changes-federal-health-spending-national-health-spending. Published October 16, 2019. Accessed November 14, 2019.
6. Centers for Medicare and Medicaid Services. Table 2 National Health Expenditure Amounts and Annual Percent Change by Type of Expenditure: Calendar Years 2011-2027. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NationalHealthAccountsProjected.html.
7. Ending the Stranglehold of Health Care Costs on American Families | Elizabeth Warren. https://elizabethwarren.com/plans/paying-for-m4a. Accessed November 14, 2019.
8. How does health spending in the U.S. compare to other countries? Peterson-Kaiser Health System Tracker. https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries/. Accessed November 14, 2019.
9. Key Design Components and Considerations for Establishing a Single-Payer Health Care System. :34.
10. Mirror, Mirror 2017: International Comparison. doi:10.15868/socialsector.27698
11. Health Care Is A Basic Human Right | Elizabeth Warren. https://elizabethwarren.com/plans/health-care. Accessed November 14, 2019.
12. Warren T. Ending the Stranglehold of Health Care Costs on American Families. Medium. https://medium.com/@teamwarren/ending-the-stranglehold-of-health-care-costs-on-american-families-bf8286b13086. Published November 3, 2019. Accessed November 14, 2019.
13. Blumberg LJ, Holahan J, Buettgens M, et al. From Incremental to Comprehensive Health Insurance Reform: How Various Reform Options Compare on Coverage and Costs. :81.
14. 20191031_Medicare_for_All_Cost_Letter___Appendices_FINAL.pdf. https://assets.ctfassets.net/4ubxbgy9463z/2Tg9oB55ICu2vtYBaKKcVr/d124e0eeb128ad3a8d8ab8a6ccae44c0/20191031_Medicare_for_All_Cost_Letter___Appendices_FINAL.pdf. Accessed November 5, 2019.
15. Medicare_for_All_Revenue_Letter___Appendix.pdf. https://assets.ctfassets.net/4ubxbgy9463z/27ao9rfB6MbQgGmaXK4eGc/d06d5a224665324432c6155199afe0bf/Medicare_for_All_Revenue_Letter___Appendix.pdf. Accessed November 14, 2019.
16. Elizabeth Warren releases plan to fund Medicare for All, pledges no middle class tax hike – CNNPolitics. https://www.cnn.com/2019/11/01/politics/elizabeth-warren-medicare-for-all-financing-plan/index.html. Accessed November 1, 2019.
17. Pollin R, Heintz J, Arno P, Wicks-Lim J, Ash M. Economic Analysis of Medicare for All. file:///C:/Users/adamr/Documents/AciesLumen/risk/Warren%202020/Medicare_For_All_12.5.18.pdf.
18. Rosenthal E. Analysis: A Health Care Overhaul Could Kill 2 Million Jobs, And That’s OK. Kaiser Health News. May 2019. https://khn.org/news/analysis-a-health-care-overhaul-could-kill-2-million-jobs-and-thats-ok/. Accessed November 1, 2019.
19. M4A – I like It! How Do We Pay for It? https://www.facebook.com/sandersinstitute/videos/1263137220491181/. Accessed November 14, 2019.
20. Medicare Negotiation And Competitive Licensing Act An Ambitious Challenge To Biologic Patents. https://www.biosimilardevelopment.com/doc/medicare-negotiation-and-competitive-licensing-act-an-ambitious-challenge-to-biologic-patents-0001. Accessed November 14, 2019.
21. Vitals. Axios. https://www.axios.com/newsletters/axios-vitals-81be1798-7e40-41a0-8972-4d82eb6b201e.html. Accessed November 14, 2019.
22. Merck, Celgene Drugs Could Be Hit By Democratic Pricing Bill (4). https://news.bloomberglaw.com/zz-bgov/pelosi-backed-drug-pricing-proposal-targets-high-price-medicines. Accessed November 14, 2019.
23. What is value-based healthcare? NEJM Catalyst. https://catalyst.nejm.org/what-is-value-based-healthcare/. Published January 1, 2017. Accessed November 14, 2019.
24. Kagan J. What Does It Take to Be in the Top 1%, 5%, 10%? Investopedia. https://www.investopedia.com/personal-finance/how-much-income-puts-you-top-1-5-10/. Accessed November 15, 2019.
25. Sherman E. Elizabeth Warren’s ‘Wealth’ Tax Isn’t The Issue For Bill Gates And Others—The Entire Tax Package Is. Forbes. https://www.forbes.com/sites/eriksherman/2019/11/11/elizabeth-warrens-wealth-tax-isnt-the-issue-for-bill-gates-and-others-the-entire-tax-package-is/. Accessed November 15, 2019.
26. Weissmann J. The “Medicare for All” Conversation Is Surreal. Slate Magazine. https://slate.com/business/2019/11/medicare-for-all-warren-bernie-democrats.html. Published November 7, 2019. Accessed November 14, 2019.